Understanding the Stages of Liver Cirrhosis: Symptoms, Tests, Treatment, and When to Consider a Transplant
.webp)
Senior Liver Transplant & HPB Surgeon with 15+ years of clinical expertise.
17 Feb 2026

If you have been told you have liver cirrhosis, or you suspect it, one question usually comes first: "What stage am I in, and what does it mean for my future?" Cirrhosis is long-term scarring of the liver. In the early phase, many people feel almost normal. Later, symptoms and complications can appear suddenly, which is why understanding the stages matters.
Online, you will often see cirrhosis explained in four stages. Doctors also use a practical medical split: compensated (no major complications yet) and decompensated (complications have started). In this guide, you will learn both, along with warning signs, tests doctors use, treatment goals at each stage, and when transplant evaluation should be considered.
What Liver Cirrhosis Means in Simple Words
Cirrhosis is scarring that slows the liver down.
Liver cirrhosis means the liver has long-term scarring. This scarring forms after years of ongoing damage. Over time, healthy liver tissue gets replaced by scar tissue. Scar tissue is stiff, so blood cannot flow through the liver as smoothly as it should.
Your liver is like your body's "clean-up and control" unit. It filters waste from the blood, supports digestion, stores energy, and makes proteins that help your blood clot. When scarring increases, these jobs start getting affected.
Can cirrhosis stay stable?
Yes, especially in the early stages. Some people live for years with stable cirrhosis if the cause is controlled and follow-ups are regular. The key point is: stable does not mean cured. It means the liver is coping for now, and your goal is to keep it that way.
Cirrhosis Is Not the Same as Fatty Liver or Hepatitis
Fatty liver, hepatitis, and cirrhosis are related but different.
Many people hear "liver problem" and assume it means cirrhosis. But these terms are not the same:
1. Fatty liver means fat has built up in the liver. It can often improve with weight loss, better food choices, and better control of diabetes or cholesterol.
2. Hepatitis means inflammation of the liver. It can happen due to hepatitis viruses, alcohol, fatty liver disease, or certain medicines.
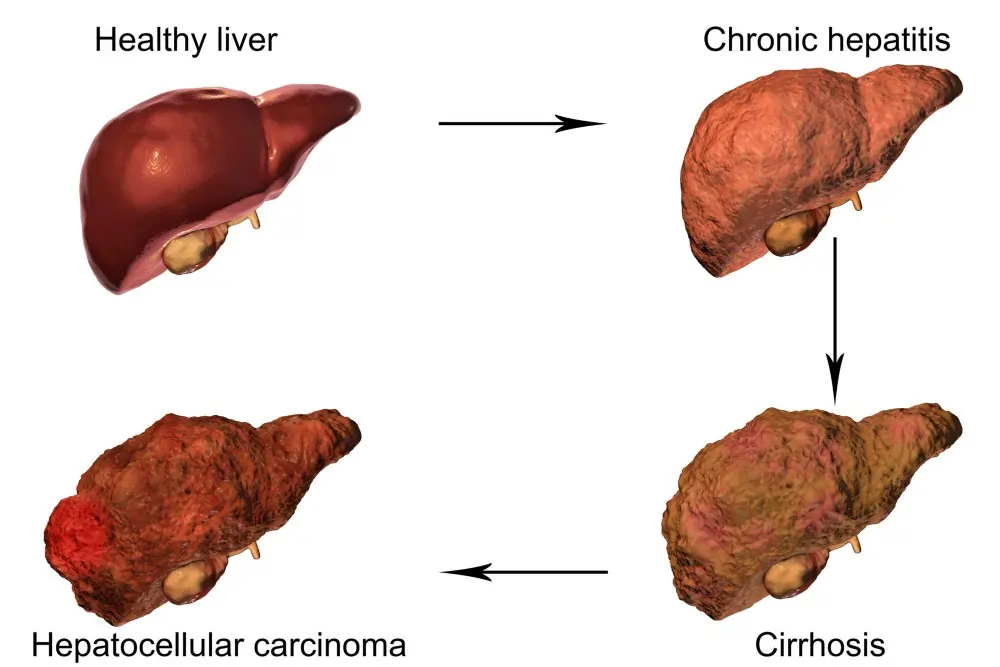
3. Cirrhosis means scarring has built up over time, and the liver's structure has changed.
Why this difference matters
Fatty liver and hepatitis can be early steps. If the damage continues for years, it may lead to cirrhosis. But not everyone with fatty liver will develop cirrhosis. Early diagnosis and action can slow damage and reduce the risk of reaching cirrhosis.
Why People Search "4 Stages" and What Doctors Use in Real Life
The "4 stages" idea is easy for patients to understand
Online, cirrhosis is often explained as having 4 stages because it feels clear and linear. It helps people understand that cirrhosis can start quietly and later cause serious complications.
Doctors often focus on compensated vs decompensated.
In real clinical care, doctors also use a practical split:
1. Compensated cirrhosis: The liver is scarred but still managing. There are no major complications like fluid in the belly or internal bleeding.
2. Decompensated cirrhosis: Complications have started, such as ascites (fluid in the abdomen), variceal bleeding, confusion (encephalopathy), or jaundice.
This matters because the moment cirrhosis becomes decompensated, the care plan becomes more urgent and more structured. Monitoring becomes tighter, and doctors may begin discussing transplant evaluation depending on severity and overall health.
Stages of Liver Cirrhosis Explained (Stage 1 to Stage 4)
Stage 1: Early scarring (often silent)
At this stage, scarring has started, but the liver still has enough healthy tissue to do most of its work. Many people have no symptoms. If symptoms happen, they are usually mild, like tiredness or low appetite. This is the stage where stopping the cause can make the biggest difference.
Stage 2: Established cirrhosis (reduced reserve)
Now the scarring is more widespread. The liver can still function, but it has less "backup." Small stresses like infections, alcohol, unsafe medicines, or poor diet can push the body into trouble faster than before. Symptoms like weakness, bloating, or feeling unwell may become more noticeable.
Stage 3: Complications begin (warning stage)
This is often the turning point. Pressure in the liver's blood flow rises, which can lead to:
1. Ascites (fluid build-up in the belly)
2. Varices (swollen veins in the esophagus that can bleed)
3. Higher risk of infections
At this stage, people often start needing hospital visits or urgent medical care.
Stage 4: Advanced decompensation (high risk)
Complications become more severe or keep coming back. People may have repeated fluid build-up, jaundice, confusion episodes, bleeding, and sometimes kidney strain. This is the stage where transplant evaluation is commonly discussed, based on severity scores, stability, and overall fitness.
Symptoms by Stage (Including Danger Signs)
Early symptoms (often easy to ignore)
In the early phase, many people feel "mostly fine." If symptoms show up, they can look like common day-to-day problems, so they get ignored.
1. Tiredness that doesn't improve even after rest
2. Low appetite or feeling full quickly
3. Mild nausea or indigestion
4. Unexplained weight loss or muscle loss over time
5. Itchy skin (can happen when bile flow is affected)
6. Sleep changes and low mood (often blamed on stress)
A simple rule: if these symptoms keep coming back and you already have fatty liver, hepatitis, or alcohol-related liver disease, don't brush them off. Early action makes a real difference.
Symptoms that suggest cirrhosis is getting worse.
As cirrhosis progresses, signs become more specific. Many of these are linked to reduced liver function and higher pressure in the liver's blood flow (portal hypertension).
1. Belly swelling due to fluid (ascites)
2. Leg and ankle swelling
3. Yellow eyes or yellow skin (jaundice)
4. Easy bruising or bleeding gums
5. Dark urine and pale stools
6. Frequent infections or fever episodes
7. Vomiting blood or passing black, tar-like stools (GI bleeding)
Symptoms of decompensation (high-risk phase)
Decompensation means complications have started. These symptoms should be treated seriously.
1. Ascites: belly becomes tight, heavy, and uncomfortable
2. Variceal bleeding: vomiting blood or passing black stools
3. Hepatic encephalopathy: confusion, forgetfulness, slow thinking, reversed sleep cycle, drowsiness
4. Severe jaundice: deep yellowing of skin and eyes
5. Breathlessness from a large fluid build-up in the belly or around the lungs
If someone starts acting "not like themselves" and has liver disease, families often think it is stress or age. It may actually be encephalopathy, and it needs medical attention quickly.
When to go to the ER immediately (do not wait)
Go to emergency care right away if any of these happen:
1. Vomiting blood or "coffee-ground" vomit
2. Black, sticky stools or fresh blood in stool
3. Sudden confusion, extreme sleepiness, or fainting
4. High fever with belly swelling (risk of serious infection in ascitic fluid)
5. Severe breathlessness or chest discomfort
6. Very low urine output or sudden swelling worsening rapidly
Tests That Confirm Cirrhosis and Show How Severe It Is
Blood tests doctors usually order (and why)
Blood tests cannot "see" scarring directly, but they help doctors understand how well the liver is functioning and whether complications are starting.
1. Bilirubin: rises when the liver struggles to process and clear bile pigments (jaundice risk)
2. INR / Prothrombin time: shows how well the liver makes clotting proteins
3. Albumin: a key protein made by the liver; low levels can signal reduced liver function
4. Platelet count: often drops when portal pressure rises, and the spleen enlarges
5. Creatinine: a kidney function marker; very important in advanced cirrhosis
6. Sodium: Low sodium can be a warning sign in decompensated cirrhosis
7. AST/ALT: show liver injury, but do not reliably tell the stage on their own
A common misunderstanding is: "My AST/ALT is normal, so I'm fine." Cirrhosis can still be present even when AST/ALT are not very high.
Imaging tests: ultrasound, Doppler, CT/MRI (what they show)
Imaging helps doctors look for signs of cirrhosis and complications.
1. Ultrasound abdomen: liver size/shape, surface irregularity, fatty changes, nodules, fluid in the belly
2. Spleen size: enlargement can suggest portal hypertension
3. Doppler ultrasound: checks blood flow direction and speed in liver vessels
4. CT or MRI: used when doctors need more detail, especially for nodules, tumours, or planning treatment
FibroScan / elastography (stiffness test)
FibroScan (or other elastography tests) measures liver stiffness. Stiffer liver tissue often means more scarring. It is useful because:
1. It is painless and quick.
2. It helps track progression or improvement over time.
3. It supports decision-making along with blood tests and imaging.
It is not perfect on its own. Doctors interpret FibroScan results along with the full clinical picture, because active inflammation, congestion, or high fat can affect stiffness.
Endoscopy and cancer surveillance (often missed, but very important)
Endoscopy for varices
If cirrhosis is suspected or confirmed, doctors may advise an upper GI endoscopy to look for varices (swollen veins) in the food pipe or stomach. Varices can bleed without warning, so finding them early can prevent emergencies.
Surveillance for liver cancer (HCC)
Cirrhosis increases the risk of liver cancer, which is why doctors often recommend regular surveillance. This usually includes:
1. Ultrasound at fixed intervals
2. Sometimes, an AFP blood test, depending on your doctor's protocol
Surveillance does not mean you have cancer. It means doctors are watching closely so any problem is caught early, when treatment outcomes are better.
Scores Doctors Use (Explained Simply)
Child-Pugh Score (A, B, C): a quick severity check that doctors use
Doctors use the Child-Pugh score to understand how well the liver is coping and how advanced cirrhosis is. It looks at a mix of blood test results and visible complications.
It usually includes:
1. Bilirubin (jaundice marker)
2. Albumin (a protein made by the liver)
3. INR / clotting time (how well the liver makes clotting proteins)
4. Ascites (fluid in the belly: none, mild, severe)
5. Encephalopathy (confusion episodes: none, mild, severe)
Based on the total score, patients are grouped into:
1. Child-Pugh A: liver is still coping fairly well (often compensated)
2. Child-Pugh B: moderate severity, higher risk of complications
3. Child-Pugh C: advanced severity, high risk, closer monitoring needed
This score helps guide treatment intensity, follow-up frequency, and planning for complications.
MELD-Na Score: often used for transplant decisions and risk prediction
The MELD-Na score helps estimate short-term risk in people with advanced liver disease. It is also widely used in transplant evaluation and decision-making in many settings.
It mainly uses:
1. Bilirubin
2. INR
3. Creatinine (kidney function)
4. Sodium (important in advanced cirrhosis)
Why kidney numbers matter: In advanced cirrhosis, kidney strain can happen even if the kidneys were previously normal. A rising creatinine and falling sodium can be warning signs that the body is under stress.
One simple way to understand it: the higher the MELD-Na score, the more urgent the situation tends to be, and the closer the monitoring usually becomes.
Treatment Goals by Stage (What Usually Changes)
Early stage (compensated): stop the cause and slow the damage
In compensated cirrhosis, the liver still has reserve. The biggest goal here is to stop ongoing injury and protect the remaining healthy tissue.
Common actions include:
1. Alcohol: complete stop if alcohol is a cause or contributor
2. Hepatitis B or C treatment when relevant
3. Fatty liver control through weight reduction, better sugar control, and activity
4. Reviewing medicines to avoid liver-toxic drugs
5. Vaccinations recommended by the doctor (often hepatitis vaccines, flu, etc.)
6. Regular monitoring: blood tests, scans, and sometimes endoscopy
Many people want a single medicine to "cure" cirrhosis. In reality, the most powerful treatment is often controlling the cause and preventing complications before they start.
Later stage (decompensated): manage complications and prevent emergencies
Once complications appear, treatment becomes more structured and often involves long-term plans.
Managing ascites (fluid in the belly)
Doctors may advise:
1. Salt restriction (this matters more than most people expect)
2. Diuretics (water tablets) as prescribed
3. Paracentesis (fluid drainage) in some cases
4. Monitoring weight, swelling, and kidney function regularly
Preventing or treating variceal bleeding
Depending on findings:
1. Medicines that reduce bleeding risk
2. Endoscopy for varices evaluation and treatment when needed
3. Clear guidance on when to seek emergency care
Managing encephalopathy (confusion)
This often involves:
1. Medicines that reduce toxin build-up in the gut
2. Treating triggers like constipation, infection, dehydration, bleeding, or certain sedatives
3. Family education, because families usually notice early confusion first
Infection prevention and early treatment
Cirrhosis can reduce immune strength. A "small fever" can become serious fast. Doctors often advise a quick evaluation for fever, belly pain, or sudden weakness.
Diet, Lifestyle, and Medicine Warnings (Practical and Clear)
Salt rule (especially if swelling or ascites)
If you have swelling or ascites, salt is not just a "health suggestion." It directly affects fluid build-up. Even strong medicines may not work well if salt intake stays high.
Practical points:
1. Avoid adding extra salt at the table
2. Reduce packaged foods (chips, pickles, sauces, ready meals)
3. Read labels for sodium where possible.
4. Use spices, lemon, herbs, and home cooking to keep food tasty.
Protein in cirrhosis: clearing a common myth
Many patients are told, "Stop protein," and they start eating less, which leads to muscle loss and weakness. In many cirrhosis patients, adequate protein is important because muscle supports recovery and helps the body handle illness better.
Doctors may adjust protein only in specific situations, usually when confusion episodes are frequent and severe. Even then, the solution is often managed protein, not "no protein."
Alcohol is a strict no.
Even small amounts can accelerate damage or trigger complications. If alcohol is involved, the safest amount is zero.
Avoid unsafe medicines and random supplements.
Some common risks:
1. NSAIDs and painkillers may worsen kidney function and fluid problems in cirrhosis.
2. Herbal "liver tonics" and supplements can be unsafe or contaminated.
3. Sedatives and sleeping pills can worsen confusion in some patients.
Always check with your doctor before starting anything new, even if it is "natural."
Safe activity and daily routine
1. Light to moderate activity is usually helpful if the doctor allows it.
2. Avoid long fasting unless advised otherwise.
3. A good sleep routine matters, especially if the sleep cycle is disturbed
When to Consider a Liver Transplant Evaluation
Signs you should not delay evaluation
Transplant evaluation is not only for "end-stage." It is often safer to evaluate early so you have time to plan and avoid last-minute emergencies.
Common triggers include:
1. First episode of ascites
2. Any variceal bleeding
3. Repeated confusion episodes
4. Rising severity scores or frequent hospital visits
5. Worsening quality of life despite proper treatment
6. Doctors are noticing a declining liver reserve in tests.
A key reassurance: Evaluation does not mean you need surgery immediately. It means you are preparing, understanding options, and staying ahead of risk.
What happens during a transplant evaluation (simple overview)
Most transplant evaluations include:
1. Detailed blood tests and imaging
2. Heart and lung fitness checks
3. Infection screening
4. Nutrition and strength assessment
5. Counselling and family discussion
6. Planning next steps based on urgency and suitability
Even if a transplant is not needed now, the evaluation often helps patients understand their stage clearly and sets a safer roadmap.
FAQs About Liver Cirrhosis Stages (Quick, Clear Answers)
Can liver cirrhosis be reversed?
Cirrhosis scarring is usually permanent, but progression can often be slowed or stopped if the cause is treated early. Some early changes may improve, and symptoms can improve a lot with the right care.
How long can someone live with compensated cirrhosis?
Many people live for years with compensated cirrhosis, especially when the cause is controlled, and follow-ups are regular. The outlook varies based on the cause, severity, and whether complications develop.
What are the first warning signs that cirrhosis is getting worse?
Common early warnings include increasing tiredness, poor appetite, weight loss, swelling in the legs, belly swelling, or yellowing of the eyes. Confusion, bleeding, or fever are more urgent warning signs.
Is stage 4 cirrhosis always terminal?
Not always, but it is serious. Stage 4 often means advanced complications, and many patients need close monitoring and sometimes transplant evaluation. With expert care, complications can be managed, and outcomes can still improve.
What foods should I avoid in cirrhosis?
If you have swelling or ascites, avoid high-salt foods like chips, pickles, packaged snacks, and many ready-made sauces. Also, avoid alcohol completely. Your doctor may also guide you on protein, fluid, and sugar control based on your case.
Can I exercise if I have cirrhosis?
In many cases, yes. Light to moderate activity can help maintain muscle and energy. But activity should be planned based on symptoms, swelling, and overall fitness. Always follow your doctor's advice if you have severe breathlessness, weakness, or frequent complications.
Can cirrhosis cause mental confusion?
Yes. When the liver struggles to filter toxins, some people develop hepatic encephalopathy, which can cause confusion, slow thinking, drowsiness, or personality changes. This is treatable but needs quick medical attention.
When should I worry about belly swelling?
If belly swelling is new, increasing fast, painful, or comes with fever or breathlessness, it needs urgent medical evaluation. Sudden swelling can signal infection or worsening ascites.
When do doctors usually discuss liver transplant evaluation?
Often, after the first major complication, such as ascites, variceal bleeding, or confusion episodes, or when severity scores rise. Evaluation early is usually safer than waiting for repeated emergencies.
Does normal AST/ALT mean cirrhosis is not serious?
Not necessarily. AST/ALT can be normal or mildly high even in advanced cirrhosis. Severity is judged using liver function tests, complications, imaging, and scoring systems.
What to Do Next (Doctor-Led Summary + Clear Next Step)
Liver cirrhosis is a long-term scarring process. In the early stages, many people feel fine, which is why it often goes unnoticed. But cirrhosis can shift from a stable phase to a high-risk phase when complications begin. Understanding the stages is not about fear. It is about planning.
If you remember only a few points, make them these:
1. Early cirrhosis can be stable for years if the cause is controlled.
2. The real turning point is decompensation, when complications like ascites, bleeding, jaundice, or confusion start.
3. Tests like blood work, ultrasound, FibroScan, endoscopy, and scores like Child-Pugh and MELD-Na help doctors judge severity.
4. Once complications appear, it is safer to manage them early and discuss transplant evaluation on time, instead of waiting for repeated emergencies.
If you or your family member has cirrhosis symptoms, a clear next step is a structured evaluation: confirm the stage, understand the cause, check severity, and create a plan that prevents hospital emergencies.
References
- EASL Clinical Practice Guidelines: Management of patients with decompensated cirrhosis (2018)
- Baveno VII Consensus: Portal hypertension in cirrhosis (Journal of Hepatology, 2022)
- AASLD Practice Guidance: Portal hypertension and varices in cirrhosis (Hepatology, 2023/2024)
- British Society of Gastroenterology: Ascites in cirrhosis guideline (Gut, 2021)
- EASL Clinical Practice Guidelines: Hepatic encephalopathy (2022)
- NICE NG50: Cirrhosis in over 16s assessment and management (updated)
- AASLD Liver Fellow Network: Outpatient management of cirrhosis (2024)